
Tag: Crystal Yormick
-

Medford slated for $2.4 million in park renovations across 26 projects
Medford is spending $2.4 million to refurbish parks and open spaces across the city. The projects range from planting trees, renovating a concession stand and constructing a natural play area to performing an archaeological dig and making accessibility improvements. The…
-

Medford mini-forest aims to reduce heat, increase biodiversity
A volunteer-run nonprofit is planting a mini-forest at Tufts Park to increase Medford’s tree canopy and biodiversity. The mini-forest will cover about 1,100 square feet at Tufts Park, a popular off-leash dog park site. Work is under way, and planting will…
-
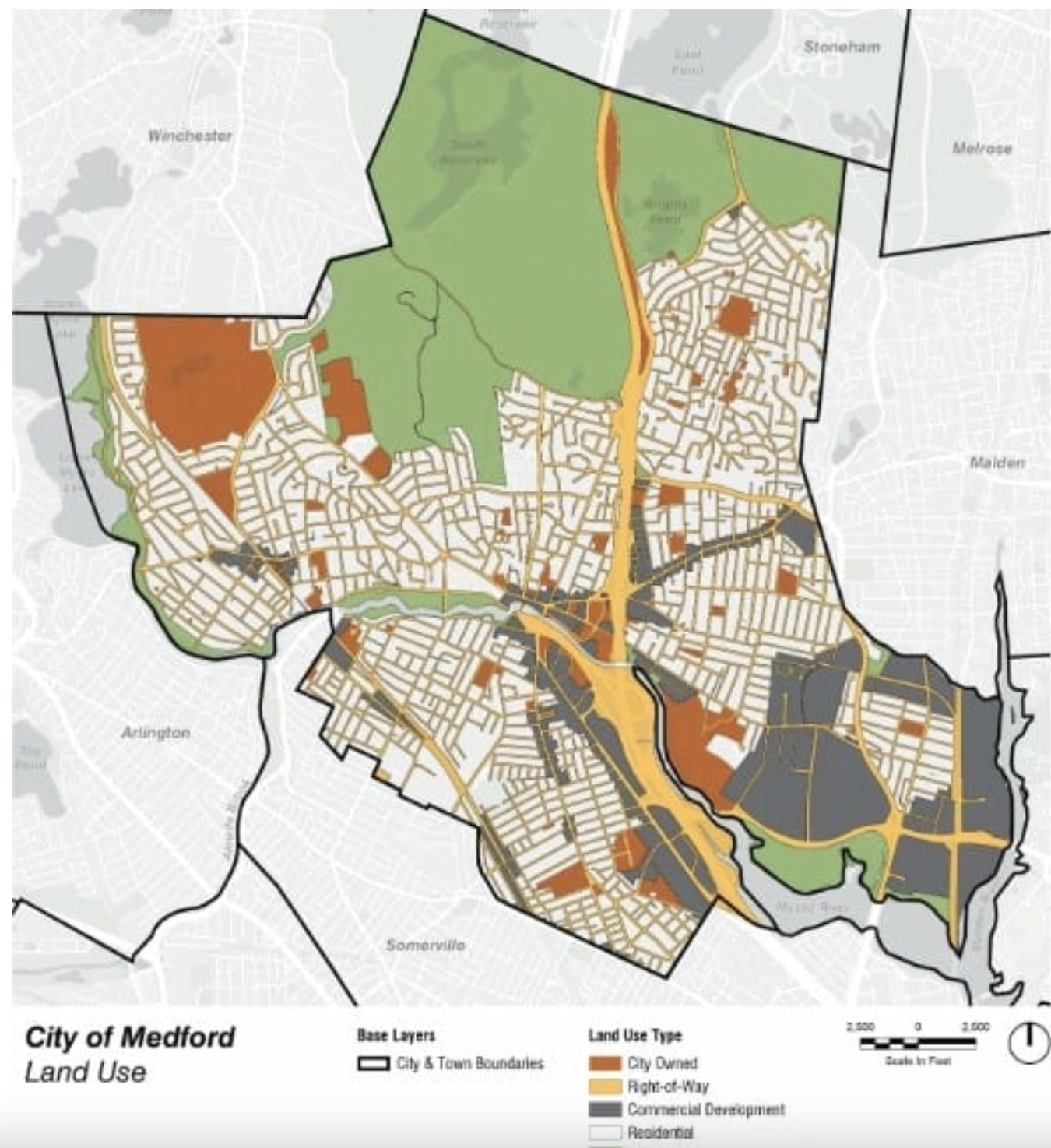
Medford’s urban forest needs some TLC and some funding, according to a new report
Graphic created by Weston & Sampson for Medford’s Urban Forest Management Plan shows current land use in the city. COURTESY/City of Medford and Weston & Sampson Medford should focus on growing, protecting and maintaining trees as key strategies for creating…
-

Tufts Medicine Behavioral Health Hospital opens next month
Courtesy Photo.
-
Medford’s Edify Church drive provides clothing for community, exposure for church
Sweaters, coats, dresses, shoes and bags line the walls, shelves and tables of the basement of a building on High Street. Although the selection features gently used items as well as clothing with the tags still attached, it is not…
-
MA nursing vacancies back to pre-COVID levels. Is that enough? ‘Normal was not great’
While nurses and hospital leaders say it’s a positive that there’s been a recent decline in nursing vacancies, they also say there’s still work to do. New data from the Massachusetts Health & Hospital Association (MHA) show that one in every 10 nursing positions is…
-
MA rent control opponents say initiative would hurt small landlords
Advocates for small property owners describe the rent control proposal likely headed for next fall’s ballot as the most “restrictive and aggressive” the state has seen to date, and say it would be detrimental to small landlords. Small property owners…